HSN Use Case
The following is a use case for the HSN functioning as the sole SIGMA+ adjunct to public health entities.
Within a period of a few weeks in early summer, public health entities monitoring the HSN in a major US city notice an unseasonable and significant increase in wearable sensor-based alerts for respiratory illness. Local providers and hospitals are not yet reporting increases in visits or hospitalizations for respiratory illness, and syndromic surveillance is not indicating increases in over-the-counter cold and flu medication. Alerts begin to show clustering in more densely populated neighborhoods.
Public health entities issue an alert to local providers and hospitals to be vigilant for respiratory illnesses and to test suspected cases for viruses such as influenza and respiratory syncytial virus (RSV). People receiving alerts begin reporting to providers for evaluation and testing, and testing is negative for common respiratory pathogens. Isolate samples are sent to state public health laboratories for testing, and results are inconclusive. Isolates are sent to the Centers for Disease Control and Prevention, and public health entities begin case investigation interviews with affected persons to determine potential exposures and timelines, monitor symptoms, and characterize interaction networks.
Deployment of an HSN affords the following benefits:
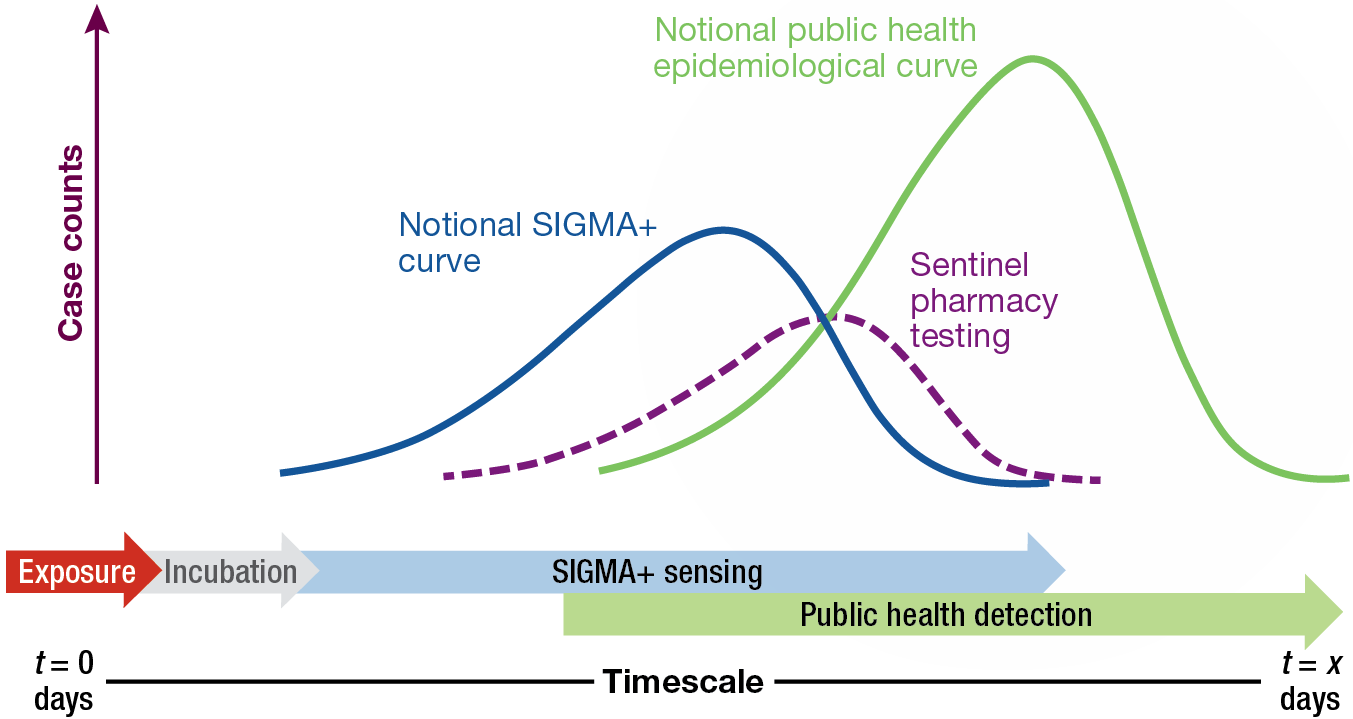
- Even without positive diagnoses, the HSN can provide early warning of unusual disease activity to public health entities, permitting prompt and proactive investigation (including coordination with local care providers and hospital systems). This, in turn, enables earlier and more accurate determination of the seriousness of the situation.
- Temporal and geographic data in combination with testing results may be modeled to estimate asymptomatic infection rates, attack rates, and areas at high risk of spread. These data can help refine assessments of the outbreak’s significance. Further, these data can be used for more targeted epidemiological investigations, interventions, and testing strategies and to inform the use of nonpharmaceutical interventions such as wearing masks and limiting social gatherings.
- Enabling officials to investigate, mobilize resources, and intervene more quickly will reduce the spread of the virus and subsequently decrease morbidity and mortality associated with infection.
- During the early stages of the COVID-19 pandemic, after the virus was circulating in the United States, but before positive case identifications had begun in most cities, an HSN could have provided early indications of spread in specific regions, nuanced understanding of asymptomatic rates and disease severity, and information about transmission characteristics. This information could have supported government responses to the public health emergency and helped mitigate the impact of COVID-19.
HSN Stakeholder Landscape
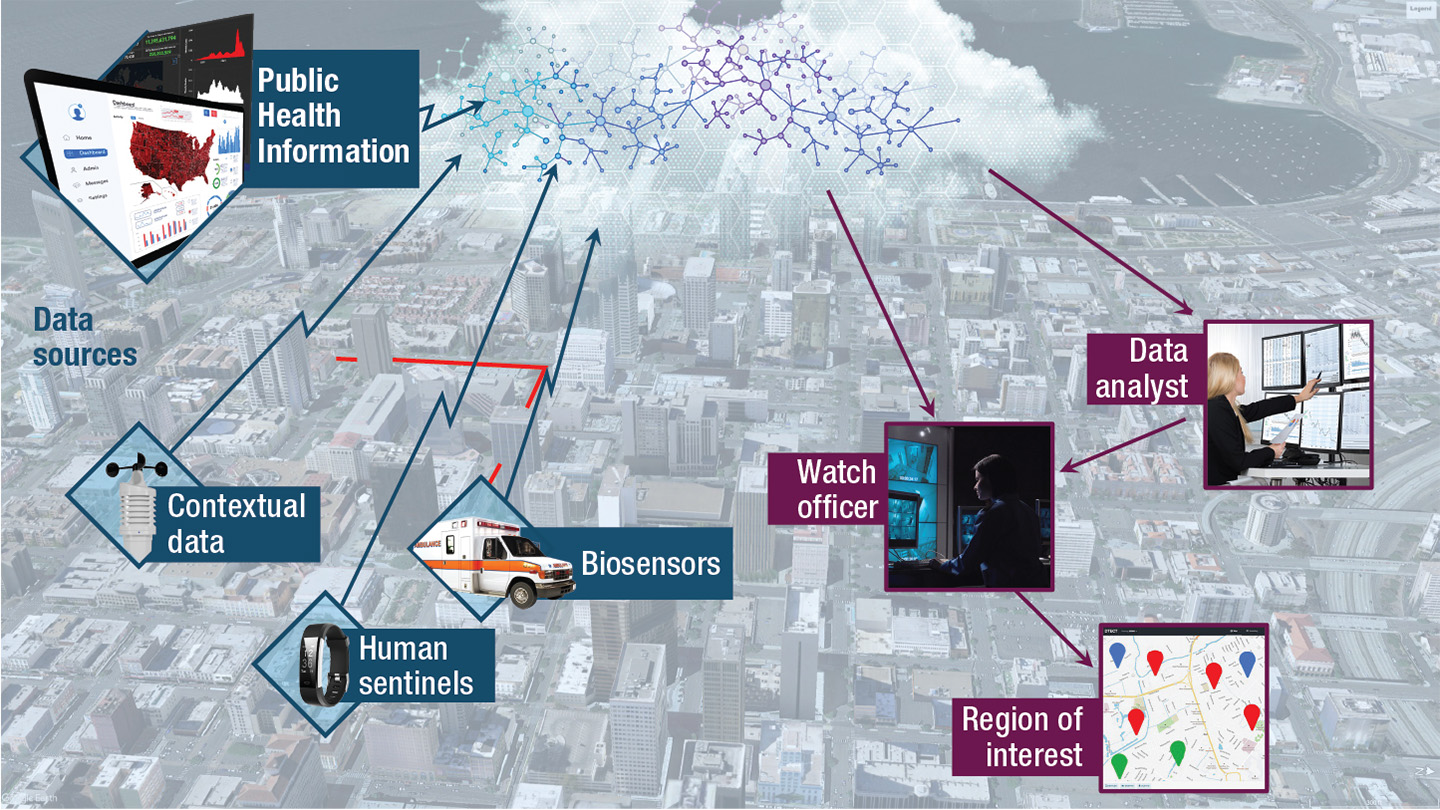
Stakeholders in a notional HSN fall into three categories: participants, data providers, and end users. Participants include individuals outfitted with wearable sensors that actively transmit data to the HSN. This group may include members of the general public, first responders, and medical personnel. Data providers are nonparticipant entities that provide relevant contextual and surveillance-related data to the HSN. These entities may include hospitals, laboratories, syndromic surveillance networks, and environmental sensors. End users include those individuals who actively monitor and leverage data and analyses generated by the HSN to make decisions in the interest of public health. End users may include people in various levels of government public health, first responders, and members of law enforcement.
Nonmateriel Considerations
Several nonmateriel factors must be considered and addressed to ensure successful HSN system design and operational deployment. These factors include participant considerations, regulations, and data protection and management.
Adequate system performance relies on a sufficient number of participating adults in the population. Approaches to achieve the required participation threshold may include government support through device donations, subsidies, or incentivization; private or philanthropic organizations, insurance providers, or wearable sensor manufacture support; and citizen science or “bring-your-own-device” participation models. Further, factors such as lifestyle, privacy beliefs, or unfamiliarity with or distrust of commercial technology may preclude certain individuals from willingly participating.
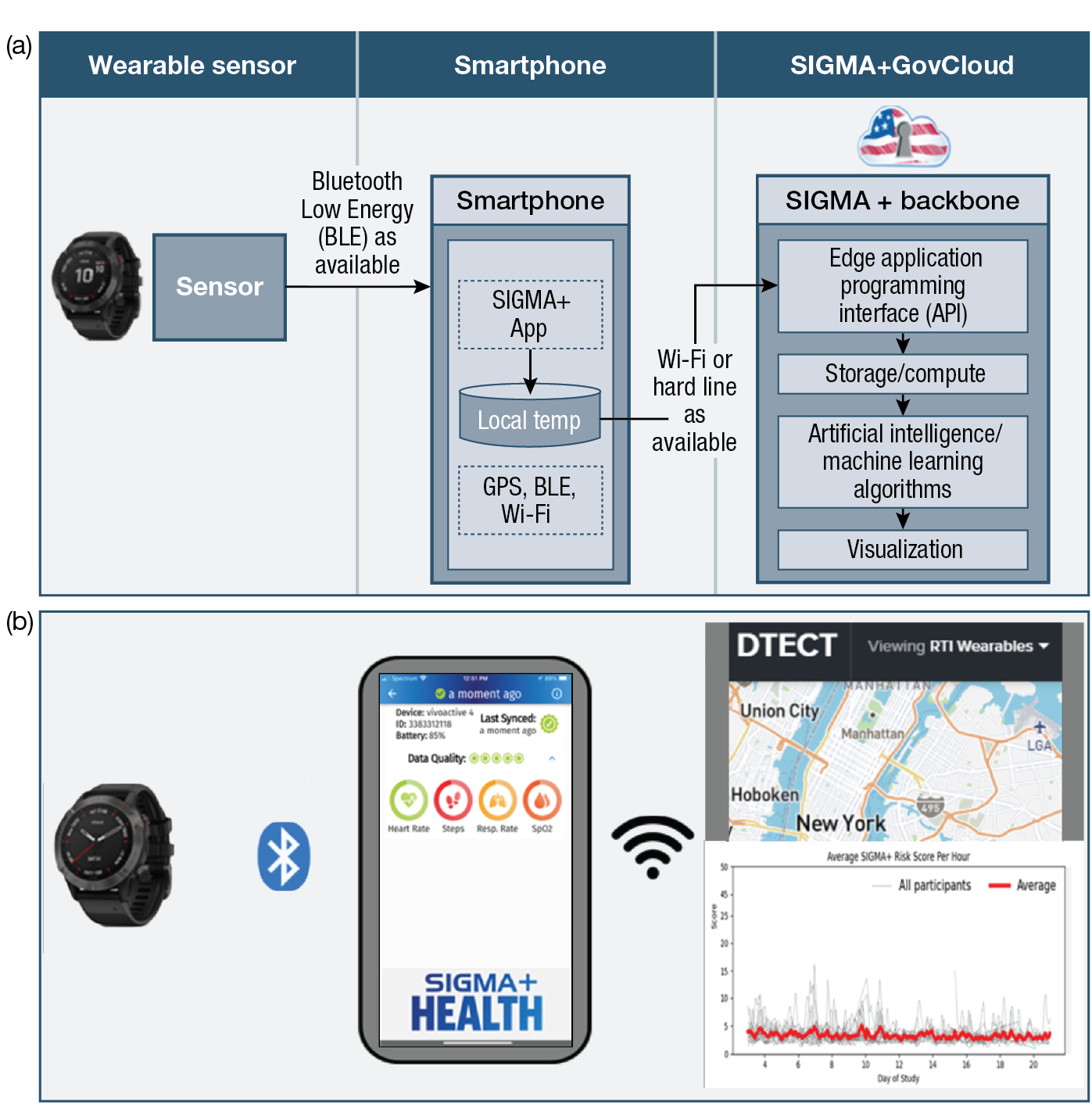
The enabling technology of the HSN is the wearable physiological sensor, which can monitor physiological attributes, track location, and communicate the collected data about the wearer. Wearable sensors may be subject to compliance with a variety of regulations (e.g., the Health Insurance Portability and Accountability Act, or HIPAA). Thorough analysis of each regulation and collaboration with relevant agencies will be required.
The protection of personal information must be the highest priority. Transparent disclosure of the types of data, how they are used, and methods for safeguarding data must be clearly communicated to would-be participants. Safeguards at the highest level of government standards must be in place to protect against inadvertent or intentional release or access. The minimum amount of data must be collected to meet system performance thresholds, and data must be anonymized as much as possible.
Feedback on the CONOPS
A significant contributor to CONOPS development was feedback solicited during focus groups and TTXs. During these events, the infrastructure and functionality of the HSN were presented, followed by targeted questions and open discussion. Feedback on the HSN fell into two categories, capability and implementation and utilization, and is summarized below.
HSN Capability
- A wearable-based, two-tier HSN is conceptually well received and would add value to emergency and public health response.
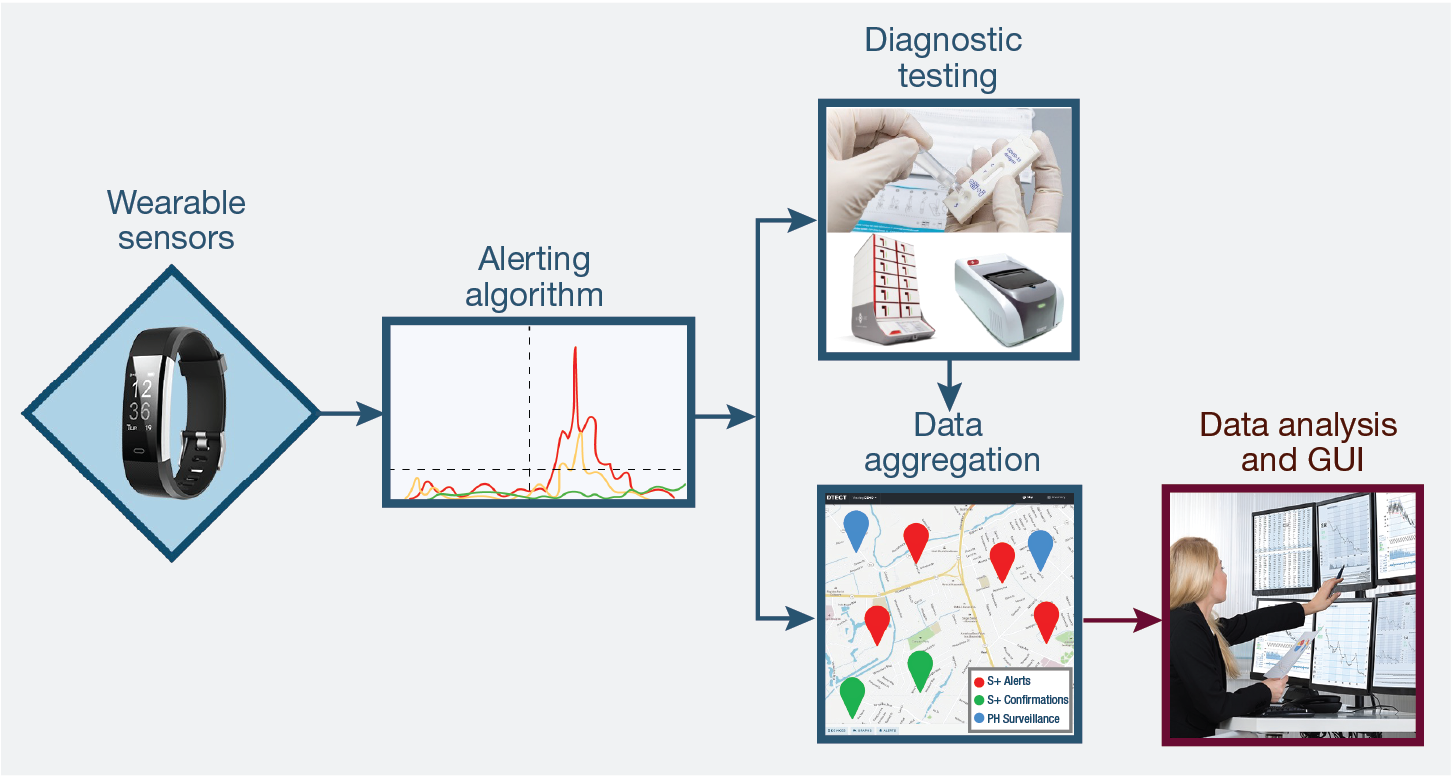
- To be effective, high-fidelity data, such as GPS tracking/back-tracking and display of the triggering physiological parameters, should be displayed for cases requiring investigation.
- When possible, data should be integrated with biosensor, agent-specific data to support response.
- The HSN provides data and situational awareness, demonstrating more utility to support broader public health response than first responders.
HSN Implementation and Utilization
- Trust in the system is critical and may be low initially while it is unproven to individual users.
- Context is important: data from disparate sources must be aggregated and presented together to provide comprehensive situational awareness.
- Jurisdictional responsibility for data monitoring and action must be determined in advance.
Summary and Implementation Considerations
Based on computational modeling and analysis, stakeholder engagements, pilot HSN studies, and CONOPS/concept of employment analysis, an HSN network is both technologically and practically feasible and would provide value to public health authorities and other decision-makers, the emergency response community, and individual participants in the network. Wearable sensors with the required features, alerting algorithms, communications networks, analysis infrastructure (including algorithms), and user interfaces are all either demonstrated or achievable with current technology. Resolution of nonmateriel concerns, including meeting regulatory requirements, is likewise viable. Any implementation of an HSN will require close collaboration with stakeholders and end users to account for locally specific factors and will require cross-agency partnerships and development of a business model ensuring sufficient public participation.
Continued development of the HSN capabilities will require interfacing with existing public health systems to test and ultimately verify, through well-defined metrics, the HSN’s ability to enhance disease surveillance. Thus, a transition partner (or partners) will likely need to conduct advanced development activities, evaluate the HSN capabilities as part of an initial operational test, conduct a pilot study of the proposed technology, and address and document full-system life-cycle challenges before deployment.
An HSN pushes the boundaries of traditional biosurveillance by providing real-time early warning updates to public health and law enforcement professionals. Information provided by the HSN will provide targeted and expedient situational awareness and subsequent decision support to mitigate the impacts of the emergency in question.
Acknowledgments: The authors acknowledge valuable contributions from the following APL colleagues: Rebecca Eager, Ariel Greenberg, James Howard, Alison O’Hare, Alex Proescher, Christina Pikas, Travis Lim, and Joseph Warfield. This article leverages insights of the following SIGMA+ collaborators: Ann Hammer and Alexis Joiner of Sandia National Laboratories; Dorota Temple and David Dausch of RTI International; Kajal Claypool and Kevin Tangen of Massachusetts Institute of Technology Lincoln Laboratory; and John Magnus and John Hungerford of Two Six Technologies. This material is based on work supported by the Defense Advanced Research Projects Agency (DARPA) under Contract No. HR0011-22-D-0001. The views, opinions, and/or findings expressed are those of the author(s) and should not be interpreted as representing the official views or policies of the Department of Defense or the US government. Distribution Statement A: Approved for public release, distribution is unlimited.