News
Johns Hopkins Uses Augmented Reality to Deliver High-Quality, Low-Cost Pediatric CPR Feedback
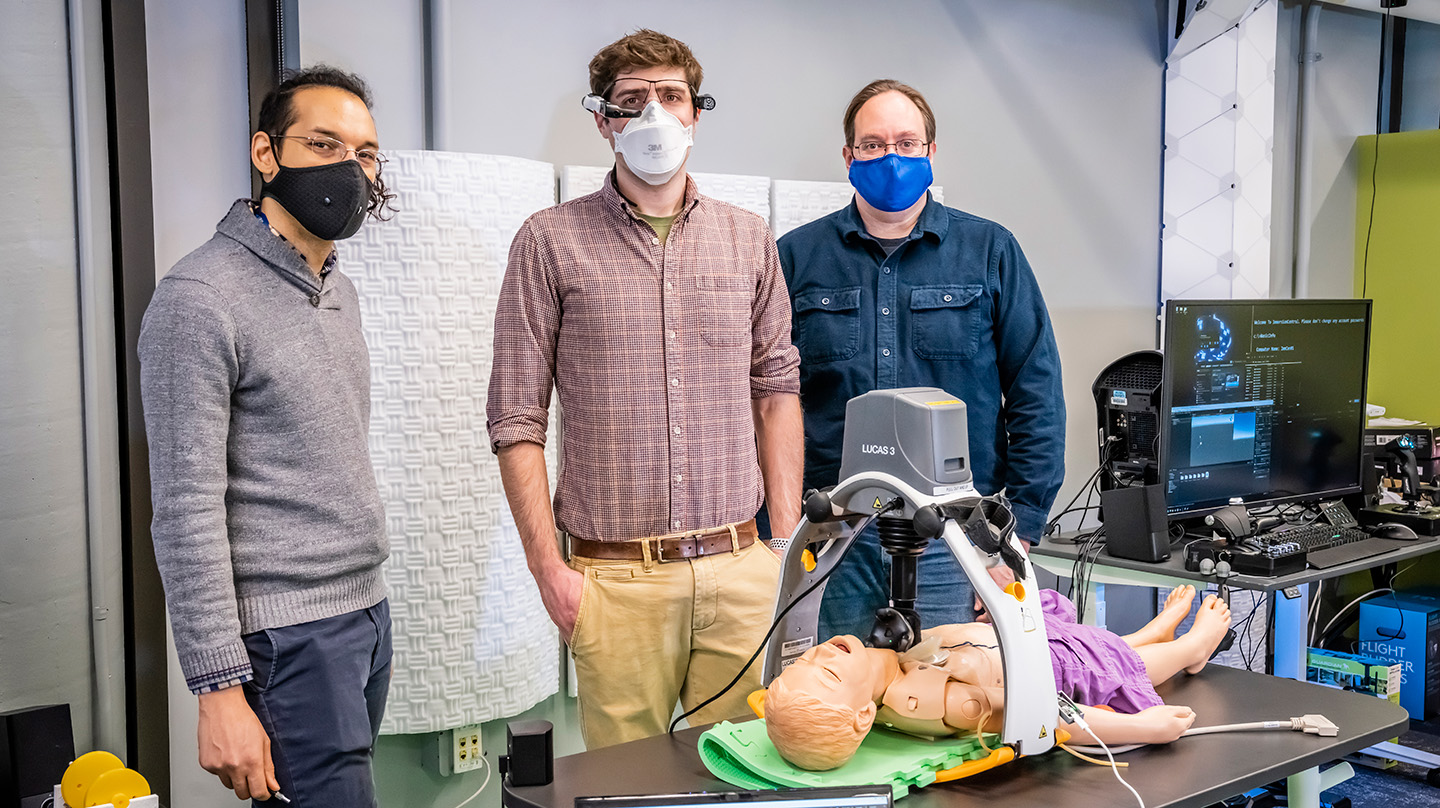
The AR CPR coaching system was developed using funding from a 2020 Johns Hopkins DELTA grant. From left to right: James Dean, Dr. Keith Kleinman and Blake Schreurs. Not pictured: Dr. Justin Jeffers, Dr. Therese Canares, Brandon Scott and Nick DeMatt.
Credit: Johns Hopkins APL/Craig Weiman
To improve the quality of pediatric CPR, immersive technology specialists at the Johns Hopkins Applied Physics Laboratory (APL) in Laurel, Maryland, and pediatric emergency physicians from Johns Hopkins Children’s Center in Baltimore are developing an augmented-reality-based CPR coaching system to be used in community care settings.
The project began under a 2020 Johns Hopkins Digital Education and Learning Technology Acceleration (DELTA) grant, designed to encourage innovation in teaching and learning.
Credit: Johns Hopkins APL/Craig Weiman
Why Real-Time CPR Feedback Matters
There are many roadblocks to successfully resuscitating children with CPR. For one, it is difficult to retain CPR training without frequent refreshers and practice, said James Dean, an immersive technology applications engineer at APL. Pediatric CPR presents an additional challenge because guidelines change with age, added Principal Investigator Dr. Justin Jeffers, an emergency medicine physician at Johns Hopkins Children’s Center (JHCC) who leads the effort and specializes in CPR and simulation training: “Those changing guidelines make it more difficult to remember and retain appropriate pediatric CPR skills.”
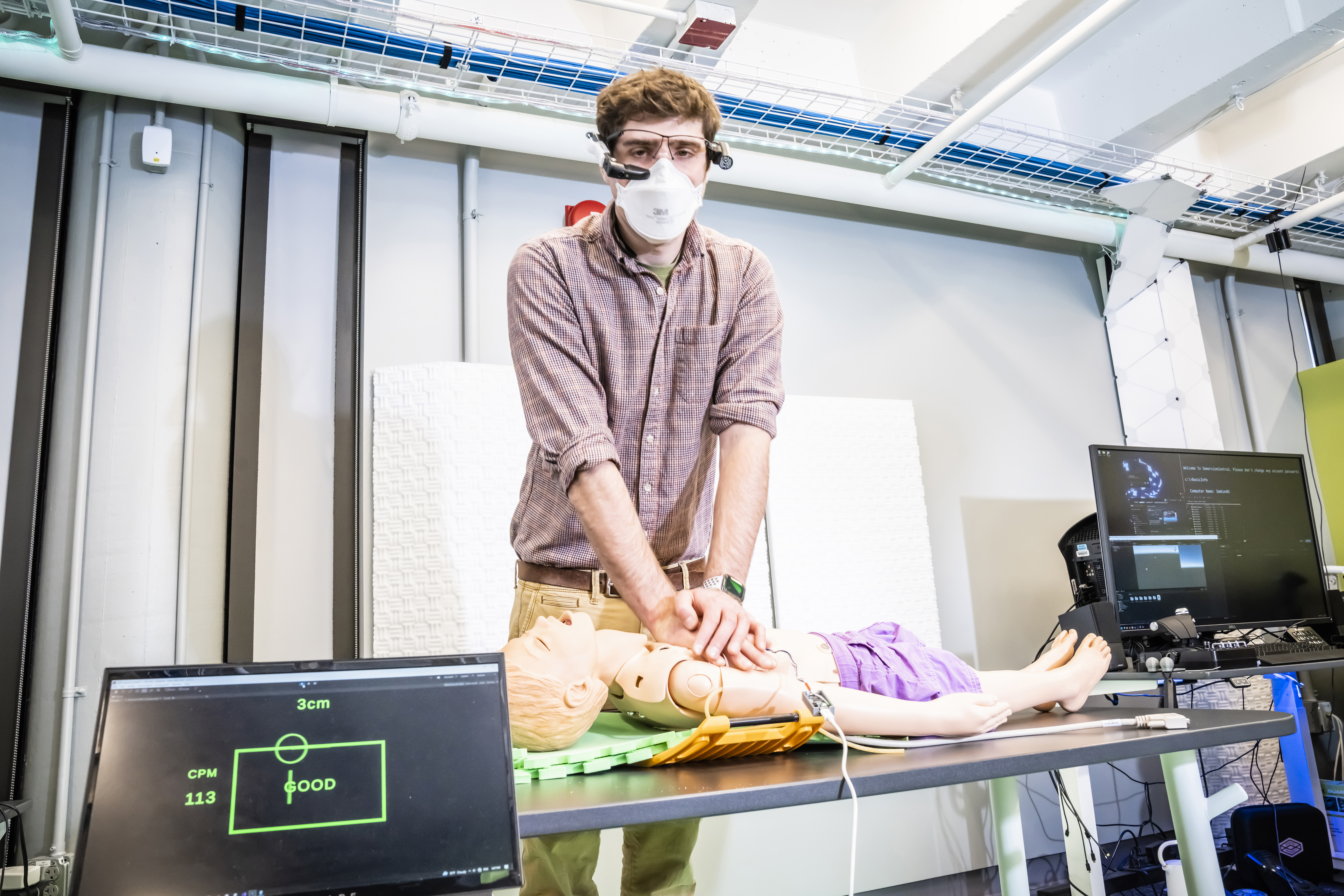
To address this problem, researchers at Johns Hopkins Medicine developed a CPR coaching system designed to provide real-time, personalized feedback to the CPR performer. Composed of a human CPR performer and human coach, the system calls for the coach to monitor a device that displays metrics such as compression rate, compression depth and chest recoil. The coach then relays verbal feedback based on those metrics to the CPR performer, who adjusts performance accordingly.
A 2018 study found this coaching system had set a gold standard for CPR quality: Following the coaching system, a CPR performer who performed simulated CPR for 18 minutes stayed within the ideal range for compression depth and rate about 60% of the time, on average. This was a marked shift from the performance of individuals unassisted by the coaching system, who stayed in the ideal ranges only about 30% of the time, on average. The study provided promising news for the more than 20,000 children in the U.S. who undergo cardiac arrest each year.
“If you’re performing CPR and someone next to you is saying what you’re doing well and what you’re not doing well, you’re going to perform at a higher quality because what you have is essentially a personal CPR trainer,” said Dr. Keith Kleinman, a fellow at JHCC involved in the study.
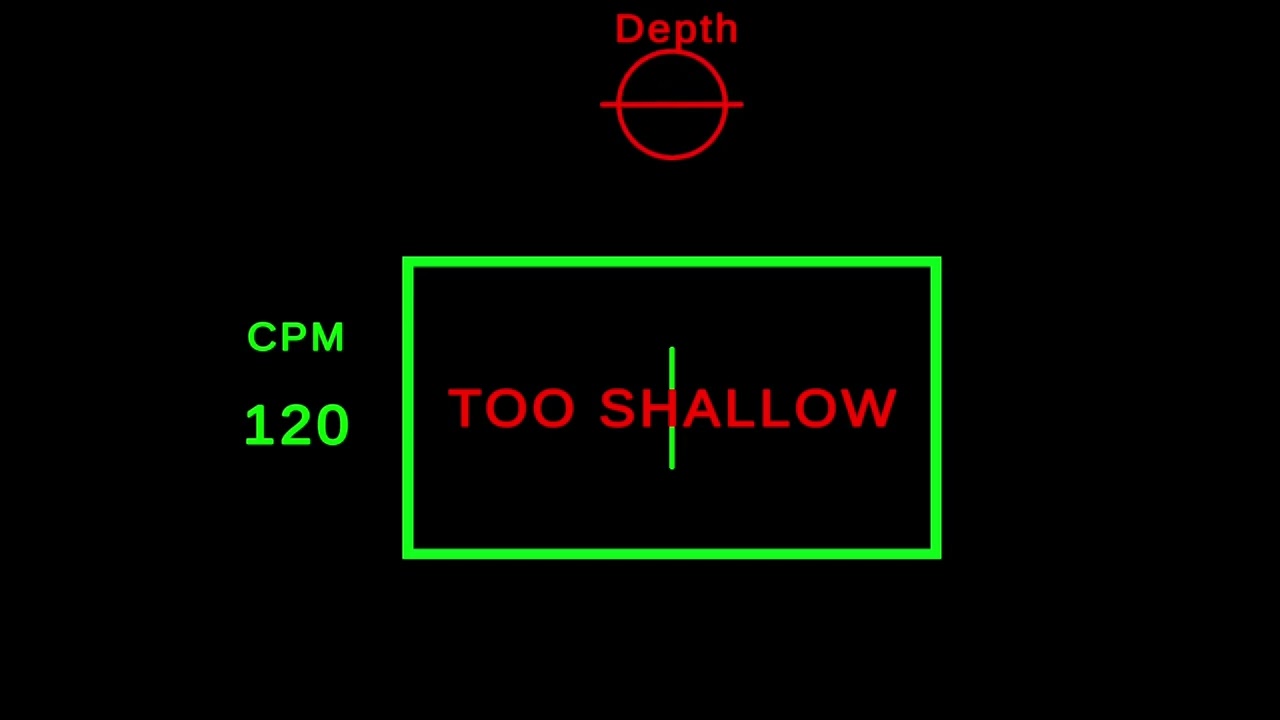
When using the AR CPR coach, the CPR performer must keep two bars — one representing compression depth and the other representing rate — inside a green box at the same time for three consecutive seconds.
Credit: Johns Hopkins APL/James Dean

In the video above, Kleinman is helping the team conduct the system’s first feasibility test at JHCC. Results suggest that when it comes to affecting human CPR performance, feedback from the AR-based CPR coaching system is comparable to that of a human-based coaching system.
Credit: Johns Hopkins Children’s Center/Therese Canares